
PIG Meeting: 18th February 2021
First Mitraclip procedure at JHH performed successfully this week!
Background
- 86 year old man
- Severe MR, 4 recent admissions to hospital with worsening CCF despite optimal medical therapy .
- Arial fibrillation, on Apixaban
- Not a suitable candidate for cardiac surgery given significant frailty and co-morbidities.
Issues
- New procedure, some uncertainty around what to expect in the perioperative period regarding vasopressor and/or inotrope requirements. Possibly some requirement for inotrope as cardiac status changing from mitral regurgitation to relative mitral stenosis.
- Anticoagulation ceased for 24 hours preoperatively in consultation with cardiologist
- Venous access using femoral vein and an atrial septal puncture, theoretically lower bleeding risk than other angiographic procedures via femoral artery
- Backup plan discussed if open cardiac intervention required – this may include valve dysfunction or embolization of device
Discussion
- Further mitral clip procedures planned in future. Note that there have been patients that have presented to perioperative clinic for other surgeries who are awaiting Mitraclip procedure. Patients should be on optimal medical therapy for heart failure prior to being considered for Mitraclip procedure.
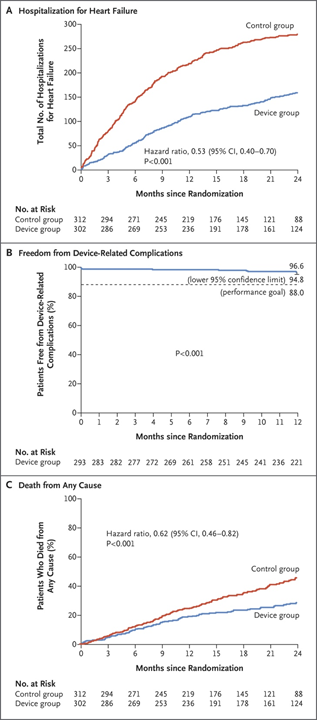
- Literature shows similar improvement in symptoms and decrease in hospital admissions with mitral clips vs open cardiac surgery. Survival benefit and improved clinical outcomes with mitral clips vs goal-directed medical management (See attached papers CO-APT trial and EVEREST trial).
Plan
- No specific perioperative interventions required than standard cardiac assessment of valvulopathy patient
- Case presented to raise awareness of potential patients presenting to pre-operative clinic
