PIG Meeting: 11th February 2021
57yo male with renal cancer for radical nephrectomy.
Background:
- BMI high ++
- T2DM
- Dyslipidaemia
- HTN
Issues
- ? Ischaemic heart disease
- Exertional chest pain
- GP arranged a stress ECG – positive
- Saw cardiologist – stress ECG again positive and the patient experienced chest pain, but stress echo negative for ischaemia. Discharged from cardiologist’s care.
- CTCA arranged which showed severe RCA vessel narrowing.
- Reviewed at cardiology-anaesthetics meeting – suggested angiogram and likely PCI.
- Discussed with surgeon –
- Will operate on aspirin but not on clopidogrel
- Based on tumour imaging suggesting nil capsular invasion, ok to delay surgery 3/12 to enable cardiac stenting and short duration DAPT.
Discussion
- Why did this patient have so many non-invasive cardiac tests?
- Usually patients have invasive cardiac testing (angiography) if one non-invasive test is positive, especially in the setting of symptoms.
- Perhaps due to GP’s strong suspicion that there was underlying IHD.
- What are the current guidelines around duration of DAPT after PCI?
- Case-by-case basis, with multiple factors influencing decision (essentially bleeding v. Stent thrombosis)
- Patient – diabetes, ACS, age, LV function
- Stent – calibre, overlaps, branching, length, DES v. BMS
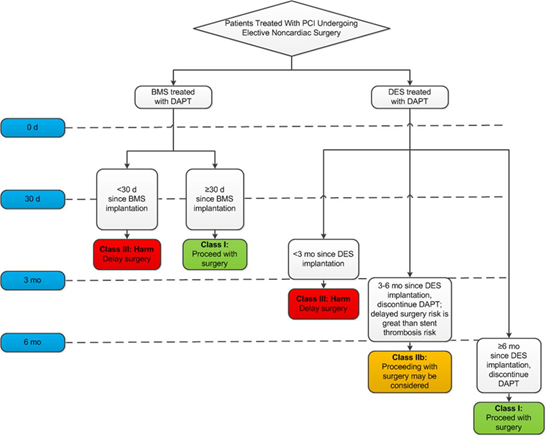
- AHA guidelines recommend 3 months of dual antiplatelet therapy post drug-eluting stent (See diagram below).
- Recent database evidence from Denmark suggests risk of MI and cardiac death after DES is elevated only with surgery within the first month after stent placement (See attached paper).
- All such cases require consultation with the treating cardiologist and surgeon to reach a compromise.
- Case-by-case basis, with multiple factors influencing decision (essentially bleeding v. Stent thrombosis)